
This blog was written by Ian Scoones and originally appeared on Zimbabweland.
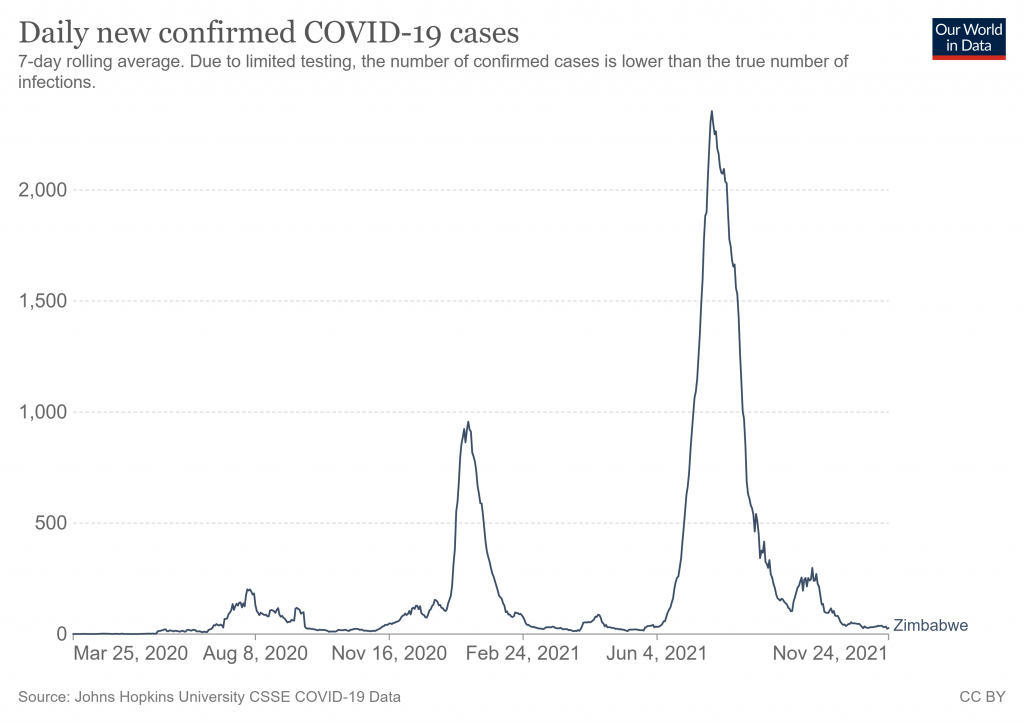
The unfolding drama of the pandemic continues. With a new variant identified in the region (Omicron) thanks to the effective work of South African genomics monitoring, Zimbabwe has been subjected to international travel restrictions. However, despite the global concern about the potential spread of what may be a highly transmissible, immune-escaping variant, things on the ground feel very different. So far at least. After the sky-high infection rates and substantial deaths of a few months back, rates subsequently declined dramatically again. Will the new variant upset this? No-one knows of course.
Conversations with our team across our sites suggests that people have been getting back to ‘normal’ life, despite some remaining lockdown regulations. What does this new normal feel like? Some quotes from across our sites illustrate. “We are now not afraid, it’s not like the early days. We know how to prevent, treat and manage the disease”. “We have indigenous remedies at our disposal. We have made so many discoveries, and now know how to fight the pandemic”. This confidence may yet be shattered by the new variant, but for now a new version of normality seems to have settled in.
While people may wear masks on transport and mask wearing gets enforced during visits to town, the situation in the rural areas is much more lax. “These masks are far too hot in this season”, someone explained. Large gatherings have started again. Political rallies are the most noticeable as electioneering starts up already in advance of the 2023 vote. “It’s the politicians who are the biggest law-breakers”, someone noted. Churches, farmers’ fairs and so on are also being held, with few restrictions and little social distancing. Curfews too, people report, are barely acknowledged especially in the rural areas. It feels, at least on the surface, pretty normal, with people making judgements about risk not in fear but with knowledge about the trade-offs and consequences.
But of course such knowledge is not certain. All can be upset with a new variant, as it has been before. And the wider context has changed too through the pandemic as livelihood possibilities have been restructured and attitudes and practices towards health and disease have changed.
Local knowledge and innovation
People repeatedly mention their discoveries of local treatments that have given the confidence in the face of disease threats. “We have done so much research”, someone observed, “we really know the situation now”. As well as COVID-19, this applies to what people call ‘cattle COVID’ too (January disease) that has struck people’s herds in dramatic fashion, often resulting in greater impacts on livelihoods than coronavirus. “We have mixed grasses, mutsviri ash and water, soaking overnight… and it works for cattle”. We are trying mutsviri ash with lemon for humans too. Along with the many remedies from local herbs to boost immunity (such as ndorani) and for COVID treatment (like zumbani), as well as the range of mixes of garlic, onions, ginger and lemon, people have a battery of treatment meaning that for now they no longer worry about the disease as they once did.
Uptake of vaccines goes hand-in-hand, with supplies now good and queues small as people take up vaccine offers. This is far from universal and to date only 18.3% of the population have received two doses. But this combination of local systems of containment and disease management with external medical intervention is seen as efficacious, and the way forward for navigating on-going uncertainties.
As experience has increased with COVID, with different waves and different impacts on different groups of people, people’s local epidemiological knowledge has increased. The seasonality of the disease is often commented on (“now it’s hot, there’s much less disease, we are not inside”); the dangers of close proximity and crowded places is clear (“even though it’s hot, I wear my mask on the combi, but not around the town”); and the dangers to those who are already vulnerable is clear (“it’s the diabetes and the BP that’s the killer – we have to eat better and consume our indigenous foods”). The revival of debates about appropriate diet (millets, not processed maize, less meat and so on) has been part of the local conversation about the disease over time.
With this knowledge comes the ability to make choices. As people commented, “in the beginning we had so much conflicting information on Whatsapp, on the internet, from friends, we didn’t know who to believe”. Now people make judgements made on experience after 18 months of the twists and turns of the pandemic, taking account of local circumstances and not taking anything at face value.
Our conversations last week happened before the new variant was identified, and this of course presents a new uncertainty that may yet shatter local confidence, returning things to dark days of just a few months back. Such is the experience of the pandemic: continuous change, continuous uncertainty.

New livelihoods
No matter what a new variant throws at Zimbabwe’s rural population in the coming weeks, the pandemic has affected the structural conditions by which people remain healthy or become sick.
Due to repeated lockdowns and the parlous state of the Zimbabwean economy, people must make livelihoods in new ways. Many businesses have closed, jobs in town are scarce and people must increasingly rely on local provisioning, especially through agriculture. There are also many new opportunities that have emerged, which have been documented in this blog series before. In urban and peri-urban areas for example, the demand for COVID treatments is met by a proliferation of new gardens, growing key ingredients. Ginger is now widely grown for example, and no longer imported from Mozambique or the Eastern Highlands. While transport has returned and farmers can move their crops to market, many have adopted new market networks, spreading risk and going for shorter transport distances, as the predatory police presence on the roads is still a problem (and a cost).
As we have documented before, many have returned to rural homes, seeking out a plot from a relative or a parent, when jobs have dried up in Zimbabwe’s cities or in South Africa. Agriculture, and especially in the land reform areas where there is more land available, is a vital source of resilience in pandemic context.
Some have taken up new agriculture-based business, switching from a town job to intensive horticultural irrigation for example, or in the case of women vendors in Chikombedzi moving into goat rearing and trade to South Africa on a huge scale. Time will tell whether this is a more permanent restructuring of the economy, but the shifts are significant and will be important for thinking about post-COVID recovery.
Autonomy and resilience
Across the commentaries from our informants in all the sites, there is a great emphasis on autonomy, and how this brings resilience. People have learned and innovated on their own. They haven’t been reliant on the state or international donors. Indeed, they have not been able to provide – the government and party doesn’t care, the donors are not interested in Africa are frequent refrains. And the competition between the Chinese, Russians and Americans over vaccines and COVID response is seen from afar with disgust.
The emphasis in local commentaries is on local adaptation through experimentation and way of responding that is localised and seemingly effective. Knowledge is shared through local networks, through Whatsapp, but is sifted now more carefully as options are considered. As people confronted the information on a new variant this weekend, according to informants there was a mix of scepticism and stoicism, but equally a sense that people were on their own as before but now with the capacity to innovate and respond.

A politics of the ‘new normal’
These new social and economic patterns of the ‘new normal’ occasionally confront the emergency focused public health efforts from the state. The emergency mode is relinquished slowly, as it serves certain interests: both political control in a volatile context and also opportunities for corruption and enrichment as lockdown laws are enforced.
There is however a distinguishable shift in our informants’ attitudes in the last month or two. With the relief that the massive peak had passed, state-enforced public health is become less accepted. Before, public health was paramount, and people mostly accepted often quite top-down, heavy-handed state intervention. The government was getting high approval ratings. It was after all a crisis, and through the news from the UK or South Africa, people also knew how bad it could get and how limited the resources in Zimbabwe were to cope with it. “We saw it on the news, we were scared.”, someone commented.
Now with less fear and more grounded knowledge along with much more experience, there is a more circumspect view, with people prepared to make judgements about risk and assess trade-offs. In the end, basic survival and the sustaining of businesses and livelihoods is important. How the arrival of a new variant will affect the assessment of risk and collective responses is of course still unknown.
Vaccine mandates
These dilemmas reflect experiences elsewhere where the limits of state intervention are being tested. There are no mass protests as has been seen in Europe and other regions, but people are also asking where does public health stop and individual liberty start? A core focus of this debate is the vaccine mandate for civil servants. In one of our study sites, a district agricultural extension office lost a significant number of staff as they refused the vaccine due to their religious beliefs being members of one of the Apostolic churches. They were put on indefinite, unpaid leave, and so effectively fired.
This has caused reverberations among civil servants, in part because for some their workload has doubled, but also they are asking whether this is fair and just. Some labour unions are contesting the decisions in the courts arguing that the vaccine mandate is anti-constitutional. Others relay concerns that this is simply the exertion of authoritarian political control, linked to a surveillance state that has no concern for liberty.
Uncertainties are everywhere
If there is one thing that this pandemic has taught all of us it is that uncertainty is everywhere and we don’t know the future. But how uncertainties are navigated and how risks are perceived does change, and we have seen this clearly through our tracking of the pandemic in Zimbabwe since March 2020 (see the previous 20 odd blogs in this series). In the last months, there has been a tangible shift in ways people are going about their lives and how they see the disease. This may yet change if the new variant strikes hard as some fear.
However, for now at least and despite Omicron dominating the headlines, most people in our rural sites across the country currently don’t spend much time thinking about COVID, as the rains have come and it’s time to plant and get on with the agricultural season. There are always other uncertainties to contend with.